
3/
PCA Stroke:
Occipital lobe → contralateral homonymous hemianopia.
Inferior temporal lobe → memory deficits.
💡 Visual symptoms may be missed !
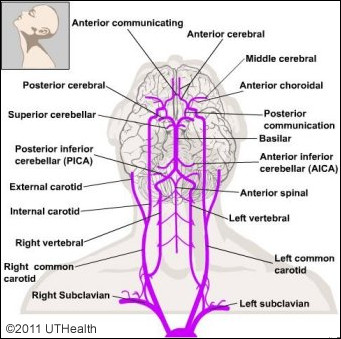
🔹 Vertebrobasilar Stroke:
Brainstem/cerebellum → cranial nerve palsies, ataxia, ‘crossed’ signs.
💡 Basilar artery occlusion → ‘locked-in’ syndrome.
PCA Stroke:
Occipital lobe → contralateral homonymous hemianopia.
Inferior temporal lobe → memory deficits.
💡 Visual symptoms may be missed !
🔹 Vertebrobasilar Stroke:
Brainstem/cerebellum → cranial nerve palsies, ataxia, ‘crossed’ signs.
💡 Basilar artery occlusion → ‘locked-in’ syndrome.
Comments
⚠️ Key Syndromes:
Watershed infarcts: Hypotension → ACA/MCA border infarcts.
PICA infarct: Lateral medullary syndrome.
💡 Know these patterns—they’re clinical game-changers!
❓ Clinical Case Quiz:
A 72-year-old has:
Right face/arm weakness
Trouble understanding speech
Which artery is affected?
A) ACA
B) MCA
C) PCA
D) Basilar
💡 Drop your answer below!
🌐 Real-World Relevance:
Stroke localisation skills save time in emergencies—helping clinicians predict deficits and triage effectively.
💬 Which clinical cases have stumped you? Let us know!
Some 🇬🇧🚑 trusts will only allow use CVA specialist pathway for anterior. My 🚑 trust we can now activate via escalation for ?posterior
✔️1st recognise they need to consider CVA in Ddx
✔️Rule out CVA mimics, eg check hypoxia & hypoglycaemia
✔️From presentation is it Ant or Post
✔️Know if pre-alert etc RE time since last seen well, anticoag etc
I had at least 3 Ddx incl this. Unfortunately, I'd limited info from that encounter
It can be frustrating as Para that its hit or miss as to closing loop for learning from case. Paramedic Postbox works well in🏥where Nurse/Dr have time @drlindadykes.bsky.social